Frequently Asked Questions
Fluoride
What is Fluoride?
Fluoride is a variation of the element Fluorine. Naturally occurring as Fluoride in nature, it is the 13th most common element on Earth. It occurs naturally in the soil and water (long before humans purposely added it to our drinking supply) and in many plants and animals, including in human body and skeletal tissues.
How does Fluoride help teeth?
- During formation: In low quantities it is incorporated into the tooth enamel during development.
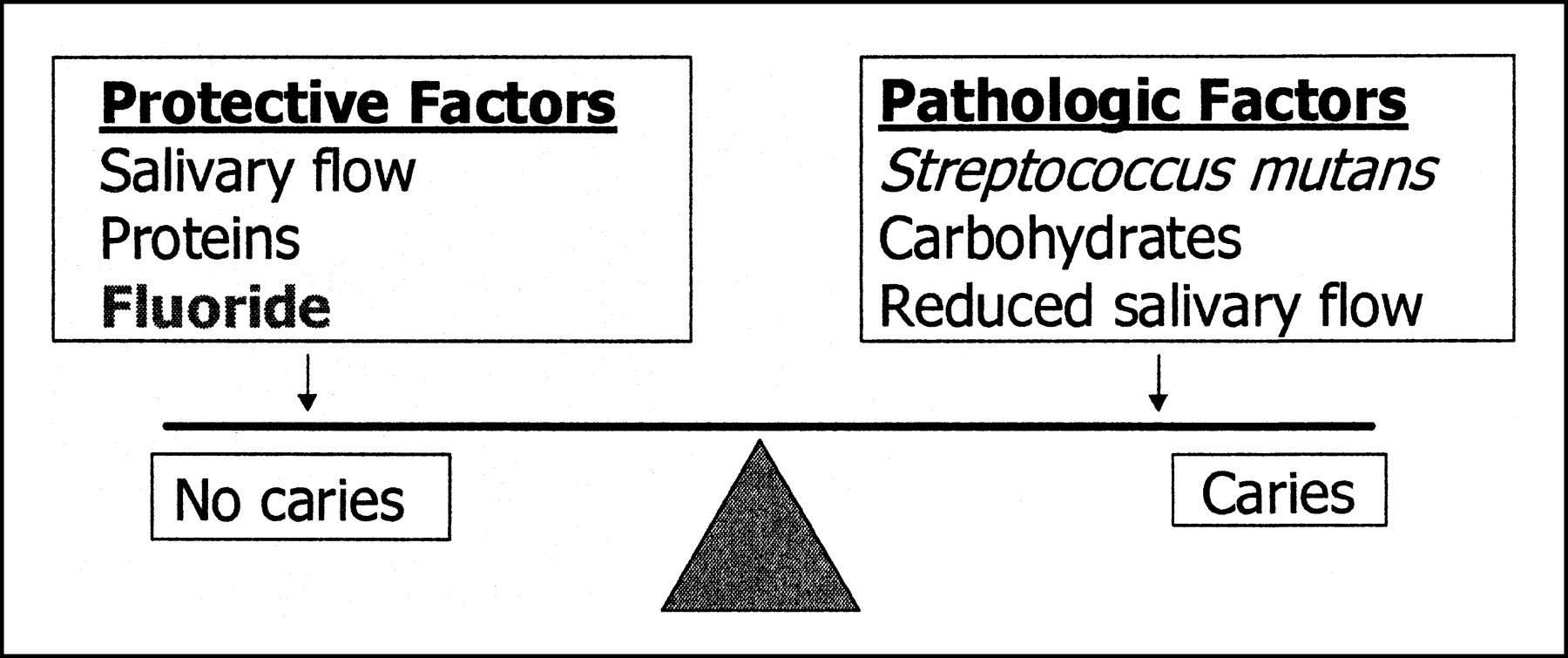
- Protection from decay: When a tooth is exposed to fluoride, a reservoir of calcium fluoride is formed on the tooth surface which can be released for remineralisation. It essentially hardens the weakened enamel in early decay.
- Antibacterial action: Fluoride has been shown to interfere with the activity and growth of decay-causing micro-organisms.
Is fluoride harmful?
Like many things in life a little bit may be beneficial, but in excess can make you sick or have side effects. Fluoride is much the same. When used as directed, it is completely safe.
Is infant formula and baby food safe?
Today the concentration of fluoride in pre-prepared formula and baby food is very low. If your baby is fed primarily powdered infant formula mixed with fluoridated water there is a slight chance for mild enamel fluorosis. While the official guidelines say that it’s safe, if you’re concerned you can alternate between fluoridated and non-fluoridated water.
Do other food and beverages contain fluoride?
Interestingly, soft drinks, beer and re-constituted fruit juices prepared in fluoridated areas will have fluoride levels very close to that of drinking water. However this does not negate the damage from the acid and sugar content. Meat and seafood are high in fluoride while some food will contain trace amounts of fluoride if they are processed in fluoridated areas.
Why is there opposition to fluoridation?
Much of this opposition stems from a lack of scientific understanding. Some people oppose fluoridation on moral grounds, considering it “mass medication” and saying that it should be their right to choose, despite the overwhelming data showing the social benefits.
What about Fluoride tablets?
Today these are considered unnecessary.
Fluoride is an essential part of dental treatment and prevention. It is used in many different forms to help keep teeth healthy and strong.
- Water fluoridation: Flouride is present on all waters to some extent, many simple chemicals are toxic when consumed in excess and the same is true for fluoride. Water fluoridation has been shown to dramatically reduce the incidence of decay by up to 40%, even in developed countries which have access to fluoridated products.
- Toothpastes: When used in conjunction with fluoridated water it has an additive effect. This should be used twice a day. Your dentist will let you know the appropriate toothpaste for you.
- Mouthrinses: The use of fluoride mouthrinses should be used in addition to (not instead of) fluoride toothpaste in those with a higher risk of dental caries.
- Flourosis or (Mottling): occurs due to a long term exposure to excess fluoride. It is found in areas with high level of fluoride occurring naturally in the water.
- Mottled or patchy looking adult teeth?
- There are a number of possible reasons for this. These range from: Molar-Incisor Hypoplasia (MIH), Fluorosis, Antibiotic Staining, Poor Plaque Control and other Formation Defects. For more information on these and other conditions and how to manage them
- Although using fluoridated water to prepare infant formula might increase the risk of dental fluorosis, most cases are mild.
- Fluorosis usually appears as very faint white streaks on the teeth. Often it is only noticeable by a dental expert during an exam. Mild fluorosis is not painful and does not affect the function or health of the teeth.
- Once your child’s adult teeth come in (usually around age 8), the risk of developing fluorosis is over.
Mottled or patchy looking adult teeth?
There are a number of possible reasons for this. These range from: Molar-Incisor Hypoplasia (MIH), Fluorosis, Antibiotic Staining, Poor Plaque Control and other Formation Defects. For more information on these and other conditions and how to manage them
X-rays
“X-rays” actually refer to the radiation emitted from the x-ray machine. The actual image produced is known as a “radiograph.” Radiographs are vital to diagnosis and treatment in dentistry. Many treatments cannot be performed (both practically and legally) without dental radiographs. The most commonly used dental radiographs include:
- Bitewings: These are the most common dental radiographs, usually taken every few years at a routine check-up or at your first visit. These help diagnose the presence of decay between the back teeth (where the dentist cannot see well), excess fillings, tartar (calcified plaque) and to help confirm the level of supporting bone.
- Periapical X-rays: These show the entire tooth, including the root and the bone surrounding the tooth. They are excellent for identifying infection at the roots of teeth and can be used to assess more extensive bone loss.
- CBCT – dental cone beam computed tomography is a special type of x-ray machine used in situations where regular dental or facial x-rays are not sufficient. It is not used routinely because the radiation exposure from this scanner is significantly more than regular dental x-rays. This type of CT scanner uses a special kind of technology to generate 3-D images of dental structures, soft tissues, nerve paths and bone int he facial region in a single scan. Images obtained with the cone beam CT allow for more precise treatment planning.
- Panoramic films (OPG): This film gives a view of the entire upper and lower jaw. It is particularly important;
- Prior to orthodontic treatment
- For patients requiring dentures and other full mouth treatment
- To assess the position of wisdom teeth
- To assess trauma and pathology in the jaw
Children’s Dentistry
The child patient is important; we at Innisfail Dentists will try to treat the patient not the tooth. Our principal aim is the freedom from pain and infection. We believe that prevention is the key for good development and maintenance of healthy and attractive primary and permanent teeth. We do try to develop child patients that are happy and cooperative.
We take pride in making their visit to the dentist as comfortable and care-free as possible. We are gentle, caring and love to joke around to help put them at ease.
Whether kids need just a simple examination and clean or something more such as fillings, fissure sealants, mouth guards or even orthodontics, we are proud to offer a wide range of services.
When should my little one have their first check-up?
The ADA (Australian Dental Association) recommends the first check-up should be at 12 months. Most little ones are uneasy sitting in the dental chair by themselves. At this early stage the visit will usually consist of “tell, show and do” and let the child go for a “ride in the chair” and generally get used to the dental environment.
It is less-than-ideal if a parent brings them to the dentist for the first time when there is a problem or pain. This association between dentist and pain can often stay with them for the rest of their lives.
My child still hasn’t got their adult tooth through? Should I be worried?
While most parents get concerned when children at school are losing teeth and their child isn’t, chances are they just need a bit more time before it’s their turn. However in instances where teeth are delayed in eruption by more than 12 months, a dentist may chose to take an x-ray to check for the presence of the adult tooth. Most of the time, the tooth is there, but in rare instances, adult teeth can be missing or impacted. Consultation with an orthodontist or even an oral surgeon may be required in this case.
Will my child need braces?
Many orthodontic problems can be detected early (although the staging of treatment depends on the type of problem). There are instances the dentists can’t predict the development of the jaws. Understand that jaws and faces grow, and issues that may seem problematic early on, may actually correct themselves with time, although some may not. The dentist can study the growth of the jaws, position and alignment of baby teeth and take into account the parents history of braces/growth to form an idea. The earliest children are sent to the orthodontist in some cases, is usually around age 8 years of age.
Do fissure sealants last forever?
Most fissure sealants will wear-away with time, but even so, the tooth with sealant is at a decreased risk of decay. The longevity depends on a number of factors including patient hygiene, grinding, diet etc.
We have special reduced prices for kids everyday preventative treatment and yes we cover children under the CDBS – Child Dental Benefit Scheme.
Amalgam fillings
Are amalgam fillings bad for you?
Most people are concerned about the mercury content in amalgam. For a person with 10 amalgam fillings, the daily amount of mercury released is 1.7μg. This is similar to trace amounts found in fruit, vegetables and eggs. By comparison a can of tuna can contain 20μg of mercury. Links to patients with health conditions including cardiovascular diseases, diabetes, cancer, Alzheimer’s disease, multiple sclerosis and Parkinson’s disease have not been proven despite numerous studies and have been rejected by the WHO (World Health Organisation) and FDI (Word Dental Federation). The only proven side effect in some people is a localised allergic reaction.
Should I replace my amalgam fillings?
Cracked amalgam filling
Unless the amalgam shows signs of chipping, cracking, leakage or adjacent decay, replacing an amalgam in a non-aesthetic area may be unnecessary. The tooth may be further weakened and/or risk becoming uncomfortable. Replacement should always be discussed with your dentist first.

Crowns

How much does the crown cost?
Please also check with your dentist in regard to cost, as costs vary depending on material and restorative requirements. Crowns are customized to fit each individual tooth and are a labour intensive process, requiring numerous hours of preparation by both the dentist and lab technician. Special materials are required to give a strong, lasting finish.
Does a Crowned Tooth Require Special Care?
Your crown may not need a special care, just the normal care you give to your ‘real’ tooth. It is however important to understand that the underlying tooth is not protected by the crown from decay and gum disease. This is why you must stick to a good oral hygiene practice.
Is it Painful to Get a Crown?
Patients will only need a local aesthetic to remain comfortable during the crowning process. There are mild toothaches and sensitivity but with painkillers, patient will be fine. But in case the pain is severe and prolonged, make sure you see a dentist.
A crown has come out. Can it be re-cemented?
Often a crown can be re-cemented, especially if it comes away cleanly and can be repositioned easily by the dentist. However if a portion of the tooth or core filling has come away with the crown it is often difficult to re-cement. Understand that if a crown comes off, it will usually not last as long as when it was originally cemented.
How will you be able to match the colour of the crown exactly?
Matching the crown/bridge to your existing teeth (or crowns) often takes some patience from the dentist and lab technician. We have a vita easy shade, a digital tooth shade measurement device for determining the shade of natural dentition, whitened teeth and ceramic restorations precisely, quickly, and independently of the ambient environment.
Some times Photographs are required (especially for front teeth) and for important/difficult cases, the lab technician may need to personally view the teeth to get them as accurate as possible.
How Long Will a Dental Crown Last?
Since dental crowns aren’t the natural teeth, they will not last forever. However, they can last a long time if good care is given to them. Research shows that more than 90% of crowns will be intact for more than five years before any other major treatment is done to them. However, 50 to 80% of crowns will last between 15 and 20 years.
Root Canal Treatment

What are the alternatives?
The main alternative to root canal is extraction. Once extracted, your options are to either leave a space (gap), or replace the tooth with either an implant, partial denture or bridge. Ask your dentist to discuss the options in more detail.
How much will it cost?
There is no “standard cost” for a Root Canal. It varies with the number of canals and overall difficulty. Your dentist will give you an estimate of the cost following your initial consultation. Please note, the final restoration is also required.
What if I have a difficult Root Canal? Is there anything that can be done?
If your dentist deems that the root canal is complex, there is always the option to see a specialist. Endodontists are specialists in RCT. They have done an additional 3 years of training in this field. Endodontists also have extremely high-tech equipment including high-powered microscopes, which allow them to see great detail and perform even difficult RCT cases. Your dentist will advise you if referral is recommended.
Why did my root filled tooth become dark?
Discolouration in some cases, the treated tooth may lose its original whiteness and become darker. If the front tooth is affected, the person may feel unhappy about the tooth’s appearance . Discolouration can be treated by bleaching, a crown or veneer can be fitted.
I’ve had Root Canal before and now the tooth is sore?
Root canal is normally around 90% successful after 10 years when performed the first time. However further decay or trauma to the tooth can cause re-infection. Specialist referral is usually required where the root canal may need to be re-treated. Other treatments may involve apicectomy (a special operation) or even investigations into external sources of pain.
Dentures
I need to have a tooth removed and I don’t want to left with a gap at all. Is there a way to have a denture put in immediately?
Yes. This is called an immediate denture. This requires advanced planning and allows a denture to be issued on the same day that teeth are extracted. Impressions and a colour-match of your teeth will be required. A denture will then be constructed and then fitted immediately following tooth extraction.
Is it possible to have a combination of denture and implants?
This is called an implant-retained over-denture: The implants (usually minimum of four in an arch) attach to the denture to hold it in place.

How long will it take me to get used to a denture?
Just like a person who has a prosthetic leg will not get up and run a marathon the first day, dentures take time to get used to. Eventually they become comfortable and most people don’t even notice they are there. Some difficulties in speech, chewing and even some rubbing may be experienced initially.
How much do dentures cost?
Dentures are a labour-intensive process designed and customised to each individual. Costs will vary depending on material used, number of retainers required and number of teeth replaced.
Denture Maintenance
Over time we may find that dentures don’t fit as well as they used to. Sometimes through accidents, or simply wear-and-tear, dentures can break, become worn or simply not fit. Other reasons for dentures not fitting include changes to teeth (e.g fillings, crowns or extractions) or other injuries. Treatment can vary from case to case.
Denture Adjustment
Sometimes a simple adjustment such as tightening a clasp or adjusting a sore spot is all that’s required.
Denture Reline
When the acrylic fitting surface ( pink plastic) of a denture does not sit flush against the gums, sometimes the use of denture adhesives can help. However if the discrepancy is too great, re-lining the fitting surface with new acrylic can help it sit more comfortably again.
Denture Repairs
My acrylic denture broke clean in two. Can’t I just glue it back together?
DO NOT ATTEMPT TO GLUE IT TOGETHER YOURSELF – it can distort the denture, affect the fit and will often become plaque retentive and irritable. It needs new acrylic to fill in the crack and allow it to fit together again.
I need a tooth out and I already have a denture. What can I do?
If a tooth adjacent to a partial denture requires extraction, you may be able to have the tooth added to your existing denture. This will depend on the denture and must be assessed on a case-by-case basis. If the tooth is important for the retention of the denture (i.e. a clasp sits around it) then a clasp may need to be added to latch around another tooth as well. In some cases a tooth addition cannot be achieved and a new denture may be required.


How much do denture repairs cost?
Denture repairs are a labour-intensive process and often require the use of a lab technician. Each repair is customised to the needs of your particular denture, and costs will vary. WE will be happy to provide a quote
The nature of the repair will depend on the damage and the type of denture. Most denture repairs will require two main appointments = the first for the impression to be sent to the lab, and the second for the issue and any remaining adjustment. Some common repairs:
- Clasp breakage: Sometimes the retentive clasp that attaches to the tooth is broken. Acrylic dentures are usually straightforward and a new clasp can be added. For metal dentures, complex metal work and re-casting may be required.
- Broken teeth: Chipped or broken teeth are usually straightforward to replace or repair. Be warned that depending on where the denture was made and/or how old the denture is, the lab may not have the exact type of tooth in stock. However they are usually able to match the tooth fairly closely. The pink acrylic they use to anchor the tooth in place may also vary.
- Broken Denture base: More common for acrylic dentures. Depending on how many pieces the denture has broken into, the denture may or may not be able to be put together. The acrylic used to repair the denture may differ in colour.
Whitening
Do toothpaste whiteners work?
Whitening toothpastes typically only clean surface stains and don’t actually change the color of the teeth. There may be some visible results but the teeth aren’t actually being whitened.
Is tooth whitening bad for my enamel?
There is no permanent damage caused to the enamel or any other tooth structures by tooth whitening.
How long does tooth whitening last?
Typically you can expect whitening to last from six months to two years, although some studies report results lasting up to 10 years. Avoiding red wine, coffee, and smoking—all of which can cause staining—helps preserve the results.
Is tooth bleaching safe?
Yes, many studies have proven that tooth whitening is safe. You can protect your tooth enamel by using calcium sulfate and fluoride.

Does tooth whitening affect fillings, veneers, or crowns?
Tooth whitening has little or no effect on restorative materials such as porcelain or crowns, but it may temporarily reduce the bond strength between enamel and composite restorations. This is why it’s a good idea to check before beginning any course of tooth whitening.
Does tooth whitening cause permanent tooth sensitivity?
Sensitivity from tooth whitening is always transient. That means if there is any sensitivity caused by the whitening, it goes away within one to two days after the treatment, and the patient returns to the state of sensitivity he or she had prior to starting the whitening process.

Intra-oral Digital Scanner
Intraoral scanners provide a level of detail of the dentition and soft tissue not previously available to oral health professionals. This improvement in image quality leads to distortion-free digital models that some doctors feel result in appliances that fit more predictably than those fabricated using conventional methods.
Better fitting appliances also result in higher quality treatment outcomes. Intraoral scanners use video or still image capture, coupled with powerful software, to take images and fabricate virtual copies of the mouth. They do not use X-rays or cone beam computed tomography (CBCT). Patients do not always understand the difference between CBCT and a virtual scan, so it’s helpful to explain the distinction.
Intraoral scanning eliminates the risk of patients gagging, an advantage for all parties involved. When the clinician performs a scan, if transient brushes with sensitive tissues occur, the clinician can simply move on and return in a more careful manner, recapturing that area after the patient has felt the accomplishment of the now nearly-complete scan. The experience is more pleasant for both the patient and the clinician than with traditional impression methods